The Impact of Seven Day Opening of GP practices on A&E Attendances
In England, the primary care physician is the General Practitioner (GP) and plays a central role in the National Health Service (NHS). The reality of the NHS service is that 90% of all contacts with the NHS are made with General Practice which remains a highly cost-effective method of delivering health care for the general population and performs a ‘gatekeeping’ function for more expensive treatment in Secondary Care.
Authors
In England, the primary care physician is the General Practitioner (GP) and plays a central role in the National Health Service (NHS). The reality of the NHS service is that 90% of all contacts with the NHS are made with General Practice which remains a highly cost-effective method of delivering health care for the general population and performs a ‘gatekeeping’ function for more expensive treatment in Secondary Care.
The GP’s role has assumed increasing importance in recent years since they now play a vital role in commissioning health care via the Clinical Commissioning Groups (CCG) created in 2014. The NHS currently faces twin pressures of financial austerity, and of continually rising demand for services. A major issue in the last 5 years has been the hours that GP surgeries are open and the extent to which this impacts on A&E services. Clearly the logic is that many patients present at A&E out of the hours that GP surgeries are normally closed – simply because then need some medical attention – even though the case may not be a medical emergency. This means the cost to the NHS is enormous. Specifically, the cost of an A&E appointment could be ten or more times that of a regular GP appointment. Therefore, it makes economic sense to open GP surgeries out of normal hours to cater for this demand. This scheme was trialed in Central London CCG and the results rigorously evaluated econometrically. The research I co-authored in the Journal of Health Economics showed that 7 day GP opening was shown to be effective in reducing A/E attendances and unplanned admissions when the services offered walk in same day access for patients, which is intuitively correct.
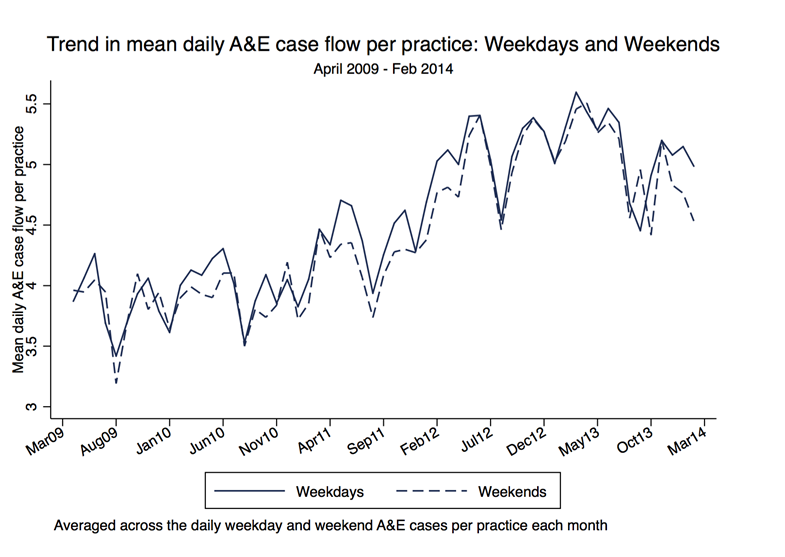
However, access to the GPs themselves has become an issue. The proportion of patients who reported finding it difficult to get a GP appointment has risen in the last 4 years. At the same time the number of A&E attendances has risen sharply from 16.5 million in 2003-4 to 21.8 million in 2013-14, a rise of 32%. (This trend in Central London CCG is graphed below.) Politicians, policy makers, and the media have all focused on GP practice opening times as both, a cause of the problem and a potential solution.
The `Prime Minister’s Challenge Fund’, was set up in 2013 to pilot seven day opening of GP practices. While the main aim was to improve access to GPs, a spillover benefit was the potential reduction in expensive A&E appointments by re-routing some patients to lower cost, routine visits to a local GP. Our evaluation of the impact of this intervention retrieves a `causal impact’ of the 7-day opening policy on A&E attendances.
We use rich administrative patient-level data – the Secondary Uses Service (SUS) data and focus on 4 Central London GP practices that started piloting 7-day opening at various points in time starting April 2013. The treatment pilots were compared to 30 other GP practices in Central London as the control group. The `treatment’ and control group GP surgeries are part of the same CCG.
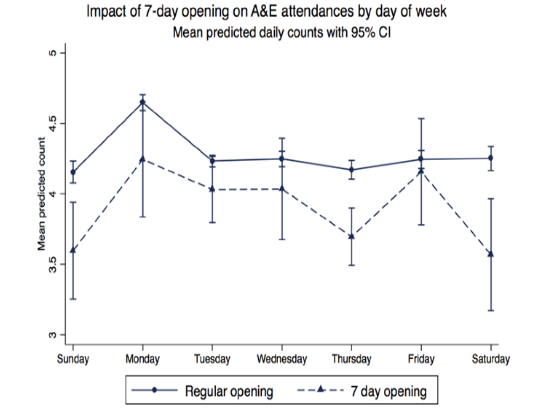
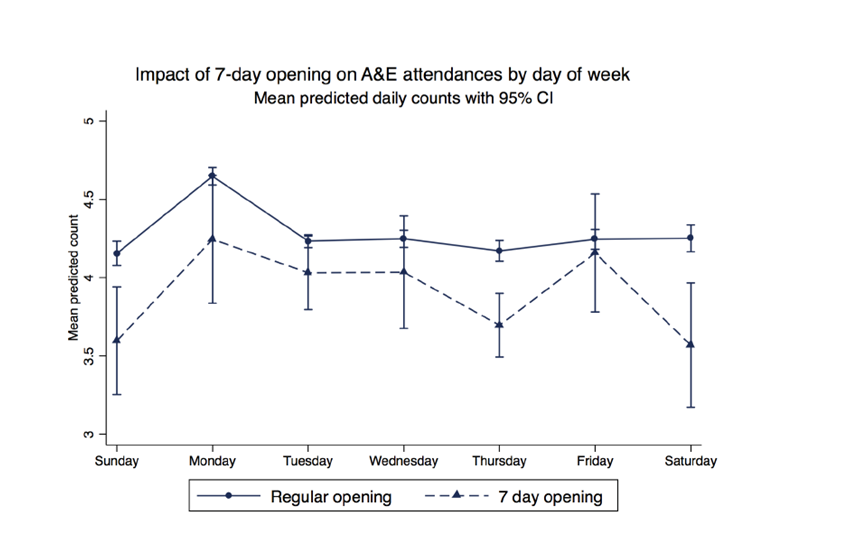
We find that the 7-day opening policy is associated with a significant and large 17.9% reduction in weekend A&E attendances from the pilots. (See the graph below). We find most of the reduction comes from a drop in cases of moderate severity. Reassuringly we find no impact on the count of A&E attendances that are induced by accidents. However, we do find an impact on A&E admissions which are also likely to be serious cases. This effect is mainly driven by an 19.2% fall in weekend A&E admissions of patients aged 60 years and above. There is a more modest drop in the least serious attendances – patients that are treated and discharged with no follow-up instructions or patients that leave the A&E without being treated. There little evidence of spillover effects during weekdays.
We also find a significant reduction of 9.9% in unplanned hospital admissions. This drop is entirely concentrated among elderly patients (over 60 years of age). This is arguably a key finding since it has significant implications for the health and well being of elderly patients, and suggests potentially large cost savings. We find that the impact of 7DO grows over time. The most plausible explanation is that it takes a while for patients to become cognisant about the fact that their GPs are now available over the weekend.
The findings are topical given the mounting crisis at A&E units across the UK and the heated political debate on the best way to tackle this crisis. In particular, our results point towards potentially large cost savings of the 7-day opening policy by re-routing a substantial fraction of patients from A&E, where a visit costs on average £114, and an admission costs £1489, to the GP where a visit costs £45.
There are potentially many implications of our findings for the way in which primary healthcare is provided. It is naive to suggest though that the problem of excess demand at A&E can be solved by simply make GPs work more hours. Given that GPs are self employed businesses, there is no current incentive for them to do so. A practice’s revenue is limited by their capitation payment i.e. under the present system there no incentive to supply extra hours. One alternative is to mandate that all GP practices should open specific regular hours and prescribe clear and transparent guidelines of out-of-hours cover. But this could significantly demotivate the existing GP workforce and could also result in a reduced supply of future GPs. One possibility to incentivise GPs to switch to 7-day opening is to re-allocate to the GPs the money saved by hospital A&Es due to reduced A&E attendances.
If the savings can be internalised, incentives could be aligned. Although recent Government plans include a 7 day GP opening service commissioned by NHS England – it specifically excludes ‘walk in’ patients and is designed only for pre-bookable routine appointments. This will not have the desired impact on A/E attendances but it will presumably make the easy political point that ‘patients can get the service they want 7 days per week’.
Related Blog Posts


What Are the Implications of the Rising National Minimum Wage and National Living Wage Rates?
19 Mar 2024
5 min read


Related Projects


Related News


Press Release: Compositional effects push up average weekly earnings at the end of 2020
26 Jan 2021
2 min read
Press Release: 2020 shaping up to be the worst year for total pay growth since 2009
15 Dec 2020
2 min read
Related Publications

Pay-Setting Among Employers in the Agriculture, Cleaning, Hospitality and Retail Sectors
11 Mar 2024
Research Report

Job Boom or Job Bust? The Effect of the Pandemic on Actual and Measured Job and Employment Growth
07 Feb 2024
UK Economic Outlook Box Analysis

Kurzarbeit/Short Time Working: Experiences and Lessons from the Covid-Induced Downturn
20 Nov 2023
National Institute Economic Review

Related events
